Is It Good to Block Endogenous Fructose Production?
In several previous posts I showed how fructose production in the liver affects metabolism through a vicious cycle of obesity. Fructose created from glucose through the polyol pathway in the liver—acts specifically via the enzyme fructokinase (KHK), which activates fructose—affects the acetylation of dozens of other enzymes through sirtuins. This makes fructose the main regulator of hepatic calorie partitioning, determining where excess energy from food is directed: either into liver glycogen or into fat, which is then sent out as VLDL to be processed by the body. In addition to regulating the allocation of calories between immediate use and transformation into fat (for storage or burning in the body), fructose also helps regulate hunger.
Blocking hepatic fructokinase makes it impossible to convert calories into fat and increases the storage of excess calories in liver glycogen. A regulatory mechanism via the brain then ensures a lower need to eat and suppresses hunger. Excesses therefore do not arise—there is nothing to store outside the liver, and no additional fat is deposited in adipose tissues.

Hepatic fructose production signals excess of consumed calories. Fructokinase is activated and fat production and calorie export from the liver to the body is preferred.
So, is it fat storage driven by overeating, or does switching calorie flow toward fat storage itself lead to overeating? I think that’s quite a fundamental question. It appears that both can be true. If the brain triggers overeating (e.g. via the hepatic signal of essential amino acid deficiency, FGF21), this activates fructokinase and directs calorie export to the entire body instead of to liver glycogen, increasing food and protein intake.
And now it depends on whether the body uses or burns these calories—or stores them. If the liver sends out the FGF21 signal, the energy will likely be burned in brown adipose tissue. This does not decrease liver glycogen consumption; food intake rises. If the calories are used by the body for ATP, hunger decreases and the overeating will be only temporary. If the calories are stored in adipose tissue, they will be “missing” for the body, liver glycogen will be consumed more, and this will lead to higher food intake. It seems that adipose tissue can fundamentally influence food intake depending on what happens with the calories within it.

Overloading and cellular senescence in adipose tissue slow down storage, increasing storage elsewhere, such as in the liver. Paradoxically, this protects male mice and extends their lifespan on a diet deficient in branched-chain amino acids (BCAAs). It prevents them from overeating like females on the same diet, who have more fat cells and are therefore more resilient. BCAA restriction triggers overeating in females and increases the risk of early death.

Back to endogenous fructose production. If we activate aldose reductase (AR) using aldehydes like HNE, this increases hepatic fructose production, calories will preferentially be sent out of the liver in the form of fats, while liver glycogen production is reduced—leading to increased food intake. So it seems we could use AR activity to regulate metabolism. If we turn it off, fat storage won’t be triggered. Would we be healthier? Probably not—why? If we turn it off by inhibiting AR, we gain nothing. Don’t believe it?
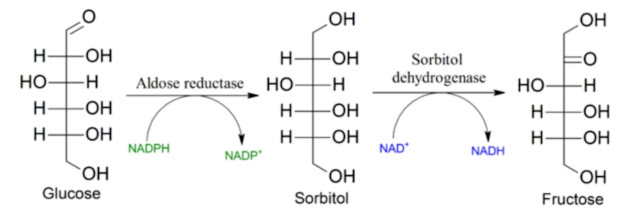
A study examining the relationship between polyol pathway activity and colorectal cancer will help us. It’s a complicated study. Let’s first look at the polyol pathway. It uses only two enzymes: AR and SORD. The study concludes that glucose or fructose alone does not increase metastasis risk; rather, it is the simultaneous action of glucose and fructose that increases the metastasis risk. Fructose makes it possible to supply NAD+ molecules for glucose-driven growth without oxygen.


We already know aldose reductase (AR)—it produces sorbitol from unphosphorylated glucose. We also know that AR, along with ALDH2, is one of the two main enzymes responsible for breaking down aldehydes, especially HNE. That’s why I consider blocking AR to be highly risky. The authors of the study claim that AR has no effect, and that cancer metastasis spreads because of dietary fructose, which is processed back into sorbitol via reverse run of SORD enzyme. Its genetic knockout (SORD KO1, SORD KO2) suppresses metastasis formation.
But this explains only part of the problem—the activation of substrate formation for growth. The reverse run of SORD consumes NADH and restores NAD+ to keep glycolysis going—that is, ATP production without oxygen. It supports aerobic glycolysis, the Warburg effect, and tumor growth.

My view is that the primary cause of cancer is unmanaged oxidative stress combined with omega-6 polyunsaturated fats. This causes cellular senescence and repairable DNA damage. Cells wait for repair and do not divide to avoid multiplying DNA damage. Cells have plenty of effective repair mechanisms—they just need energy and antioxidant protection for repair to occur. Senescence is a manifestation of a dysfunctional, oxidized superoxide dismutase (SOD) enzyme. Accumulated superoxide destroys membrane chains of polyunsaturated fats. The resulting toxins contribute to DNA damage.
If an appropriate mutation occurs, the senescent cell begins to proliferate with its damaged DNA. This is not caused by fructose itself generating oxidative stress—fructose only ignites the preexisting substrate for peroxidation. Thus sugar may appear to be a cause of colorectal cancer, but it is only a small part of the process and cannot act alone. Cancer is triggered by a substrate prone to peroxidation into aldehydes—namely linoleic acid.

And we already know that the first enzyme of the polyol pathway—AR—removes these aldehydes. Therefore we must not suppress its function; doing so would lead to cancer. We can see this in the study’s AR knockout results. The authors do not comment on it, but AR knockout (AR KO2) increases metastasis spread. Adding dietary fructose increases sorbitol levels via SORD. This could block AR function purely by increasing its product concentration and thereby reduce HNE detoxification when sugar and omega-6 seed oils are consumed together.
Let us also recall that AR is activated by SIRT1. SIRT1 activation is linked to oxidative metabolism, improved health, and enhanced resilience. This also suggests that shutting down AR is probably not a good idea for eliminating obesity or reducing endogenous fructose production. I already hinted at a better solution in the previous post: vinegar/acetate.
The study’s authors do not comment on what happens to sorbitol produced from fructose via reverse SORD activity. It must accumulate and has nowhere to go. The usual direction of SORD activity is to produce fructose from sorbitol—thus removing sorbitol—and there seems to be no alternative pathway. Cells that cannot process sorbitol have major problems with it. The figure in the study hints at diffusion through the cell membrane, but this is likely negligible.
NAD+ production for glycolysis through the conversion of fructose to sorbitol could also explain other phenomena—for example, why fructose helps lower postprandial glucose. Fructose can help supply NAD+ for glycolysis and for sirtuin activity, but increased AR activity triggered by oxidative stress and aldehydes may block this function of fructose. This could be another negative effect of high seed-oil consumption. I think there is still much left to investigate. All these phenomena should be analyzed in terms of how AR affects aldehyde detoxification at different levels of polyunsaturated fats in membranes. This could confirm or disprove the above considerations.
References:
Fructose and glucose from sugary drinks enhance colorectal cancer metastasis via SORD


Comments
Post a Comment