Is it a good idea to suppress glucose production in the liver?
Overweight and obesity are fairly common nowadays, much more common than they were, say, fifty or a hundred years ago. There are many opinions on the causes, but to me it currently appears to be the result of poisoning from food, drink, or the environment—whether the air we breathe or contamination by foreign electromagnetic signals. I assume that the environment and food simply play a role.

Let’s review the most important processes that influence fat storage and obesity.
First of all, rapid and easy storage into adipose tissue does not cause a problem and quickly removes fats from the blood. To achieve this, it is necessary to maintain metabolically healthy adipose tissue protected by the glutathione antioxidant system.
How much fat will be stored is determined by excess—some fat is constantly being burned, and excess is stored.
So it is determined by the ratio at which fats and glucose are burned. With any change in the ratio of fats and carbohydrates in the diet, suppression of fat burning or an excess of fats in the diet will mean more surplus fats available for storage. Conversely, a lack of fats in the diet will trigger higher glucose burning and the formation of fats from carbohydrates via de novo lipogenesis (DNL). I think that usually this process is triggered by endogenous fructose production in the liver, i.e., the polyol pathway. Realize that the body understands newly created fats as building material, not as fuel! Therefore, malonyl-CoA produced by DNL also ensures suppression of fat burning and conserves fats. The construction is more important.
Why do we actually eat in a way that creates excess fuel? In order to last for some time without food—for example during sleep—we must have a reserve of fuel, i.e., surplus.
There is nothing wrong with that. The main fuel sources between meals and at rest are liver glycogen and fat stored in adipose tissue. Supplying energy for movement is more or less independent of these sources. For movement functions and skeletal muscles, there are separate storage spaces for fuel—muscle glycogen and also fat stored in muscles. If these stores are filled after a meal, excess is stored in liver glycogen and in subcutaneous or visceral adipose tissue. All of this is related to how much food is available.
If we have the opportunity to consume unlimited amounts of food, our brain determines the size and need for storing surplus.
If it seems to the brain that we have had enough, it will be satisfied and suppress the need to eat. It uses various signals from the body to do this. My basic hypothesis is that the main signal for determining sufficiency, in addition to leptin produced by fat cells and ghrelin produced by the stomach, is also the level of liver glycogen. The hormone leptin is a long-term and slow signal about the amount of accumulated fat, and ghrelin is more related to stomach fullness, i.e., to food itself. But liver glycogen changes with every meal, with every short-term fast. It seems to me to be decisive for determining total daily food intake.
Redistribution between liver glycogen and export of unused fats is one of the most important functions of the liver.
It is the liver that collects excess free fatty acids (FFA) from the blood and packages them as triglycerides into VLDL particles. Part of this process is also the conversion of fatty acids into forms suitable for storage. Not all fatty acids are suitable for storage. Thus, some fats, in addition to activating β-oxidation (breaking down into acetyl-CoA molecules), also activate DNL, the assembly of new fatty acids. VLDL particles then export these modified fats throughout the body, but they are not counted in the satiety signal—as if we had never eaten them. For these fats to be at least partially accounted for, there is a sophisticated mechanism that converts them into a liver glycogen signal.
How could free fatty acids in the blood—fats not stored in VLDL particles—influence liver glycogen and satiety?
It’s simple. If excess free fatty acids are not stored in VLDL and sent away, their level in the blood increases. This activates the PPARα factor and β-oxidation of fats in the liver, more acetyl-CoA molecules are produced, and these activate the enzyme pyruvate carboxylase (PC), triggering gluconeogenesis (GNG), i.e., glucose production—more precisely, production of G6P. These molecules are converted to G1P and stored in liver glycogen.
The conversion of G6P to glucose via the enzyme G6Pase is a separate process. It is more or less part of the process of glycogenolysis and blood glucose stabilization. Only when this is not enough to cover the demand does gluconeogenesis become involved in glucose control.
It seems that glucose production by the liver is controlled by the excess of free fatty acids in the blood, which signal low insulin levels and high lipolysis. Regulation occurs such that glycerol and fats released from adipose tissue activate GNG and increase glucose and insulin production. This leads to suppression of lipolysis and a reduction in the supply of free fatty acids and glycerol to the body—a negative feedback loop, stabilizing levels at a certain point. In this way, the body directly regulates sufficient fuel supply for the resting state.
In the case of some change, e.g., physical activity or stress, additional layers of hormonal regulation are added to this system, but at rest it is the relationship between liver glucose production, insulin, and free fatty acids that controls the supply of fats and glucose for normal functioning.
In this situation, the body uses a specific ratio between burning fats and glucose, which changes depending on the duration of fasting.
The longer the fast, the less glucose will come from glycogenolysis, and metabolism will shift more toward fat burning and less toward glucose burning. Blood glucose levels remain more or less constant, being replenished by gluconeogenesis from glycerol. What changes is lipolysis and the regulation of fat burning. Production of malonyl-CoA is suppressed and CPT1A activity increases, thus increasing fat availability and transport into mitochondria. Insulin levels decrease.
Will we feel hungry in this state or not?
If the body’s needs are met, then we should not feel any deficiency—there is enough fuel in the blood, all cells can function without problems, so why would we feel hungry, for example after waking up?
Are you hungry after waking up?
I’m not. I often feel no hunger for several hours after waking. How is that possible?
If no deficiency signal is triggered, we should not feel hunger. Blood glucose levels are normal, fats are released according to how insulin and FFA regulate lipolysis. So glucose is not the signal. Fats probably aren’t either. Could the signal of deficiency be, for example, low leptin levels or leptin resistance? I doubt it—that is slow, long-term regulation and likely not closely related to the immediate need for food.
So when do we get hungry?
Blood glucose levels initially do not change, but once we hit some limit, the urge to eat will increase. The first limit is probably a lack of liver glycogen for glycogenolysis if gluconeogenesis from glycerol released along with fats is insufficient to maintain glucose levels. There will likely be a mismatch between the need for glucose production and its actual production in the liver. If we do not eat, further fasting should increase lipolysis—but that may no longer be possible. You will truly feel hungry. More glycerol and FFA will not be released, a deficiency arises, and this drives us to eat.
If your body is accustomed to fasting, your fat cells can probably release enough FFA and glycerol in time, and you will not feel deficiency, or at least not too soon. But if the body is used to a constant supply of carbohydrates, if fat cells are large or senescent, poorly functional, then they cannot supply enough fuel for fasting.
It is said that the problem is low-grade inflammation in adipose tissue, activation of the immune system. But if adipose tissue is exposed to toxins that trigger inflammation, such as endotoxin (LPS) as in bacterial infection, more free fatty acids are released. So it is rather a system for suppressing hunger.
We all know this from experience—when we are sick, even with a viral illness, we have no appetite and usually temporarily lose weight. The body lives off fats and glycerol released from fat cells. Activation of the immune system helps us live off our own body reserves.
Okay, we end the fast and eat. We consume some fats, carbohydrates, and proteins.
What determines the redistribution of calories? How many calories are stored in muscles, how many in liver glycogen, and how many in adipose tissue? Do we know? What does it depend on?
For example, this study in mice tells us how fat formation from carbohydrates can be activated and how increased fat burning can be achieved on a carbohydrate diet. See for yourself—it is achieved by applying certain restrictions.
 |
| CR - time and calorie restriction of food intake, AL - no restriction |
The principle is actually very simple—you stress the mice with deprivation, with limited time to eat.
You force them to consume their usual food in a short time window (from 0h to 2h). In order for the mice to eat more, after a few days the process of DNL is activated and more fat is created for storage even with lower overall consumption. The mice then live off this fat for the rest of the day until the next meal. It is clear that adaptation deepens even after one month of this eating pattern. Essentially, we have a pretty good model of short-term fasting.

In this eating pattern, it works and the mice thrive, but if we wanted to induce strong hunger, we would give them sugar in this situation. I think it is quite possible to reliably predict what would happen. Fructose from sugar would block fat burning and force the body to burn more glucose, which would relatively quickly reduce liver glycogen levels and trigger hunger without affecting fat stores.
Realize that with time-restricted carbohydrate intake, fat production is pushed to the maximum.
This dietary pattern changes the ratio of fat and carbohydrate burning in favor of fat burning and storage.
Fructose suppresses fat burning but does not shut down fat production!
It only shuts down fat burning by limiting CPT1a. It also suppresses antioxidant protection. Do you understand what this causes? Another cycle of time-restricted carbohydrate eating just replenishes fat stores again. More and more—just fat accumulation. While in a standard regime of gradual slow carbohydrate eating fructose is not a problem, fats are formed little and burned slowly, in a time-restricted regime the effect of fructose can be crucial.
What does this remind me of? Aren’t we taught this in school cafeterias? Or at work? You have half an hour for lunch—if you don’t make it, tough luck. That’s how I remember it from childhood; maybe it’s different now. If we are in a regime of small eating windows, what we eat matters a lot. It is good to adjust the ratio of fats and carbohydrates in the diet to the ratio of fat and glucose burning. Our timing determines fuel partitioning so that it resembles the burned ratio as much as possible. This happens via DNL, which continuously and short-term transforms acetyl-CoA into malonyl-CoA, which is then elongated to form oleic fatty acid suitable for storage. The rate of this continuous process, activation of necessary genes, is decisive.
If acetyl-CoA production from β-oxidation of fats is fast, acetyl-CoA levels rise and GNG is activated, and glycogen formation will be high. But repeating this process without glycogen consumption will trigger DNL, a continuous withdrawal of acetyl-CoA molecules. This reduces the sensitivity of GNG activation—more and more acetyl-CoA will be required to trigger GNG.
Is it a problem that GNG is not activated?
Yes, it is. Acetyl-CoA diverted into DNL is stored as fat and glycogen production is not activated by GNG. More food will be needed because part of it is stored as fat. This will trigger a feeling of hunger and deficiency sooner because DNL also limits fat burning. It seems that GNG is absolutely essential for suppressing hunger at normal blood glucose levels. At the same time, GNG must not cause cytosolic glucose levels to exceed maximum levels nor exceed the liver’s glycogen storage capacity. This system is beautifully balanced, but it must not be overloaded.
We can illustrate this with an image from the previous post. Soybean oil (blue curve) is a perfect source of acetyl-CoA, metabolized very quickly via β-oxidation. As little as 7% in the diet reliably activates GNG because it increases acetyl-CoA levels in the liver. If we do not exceed the liver’s glycogen storage capacity, this suppresses food intake. It suppresses hunger. We see this in that mice do not overeat and have low body weight. Soybean oil up to 7% (~4% dietary linoleic acid) suppresses appetite. No cannabinoid system can override this—cannabinoid receptors only temporarily fine-tune the basic regulatory system. Even gut permeability is not activated via CB1 receptors.
But just 21% soybean oil in the diet of mice (right graph) likely exceeds some limit. We do not yet know exactly which one.
My hypothesis with question marks:
Linoleic acid suppresses the export of acetyl-CoA molecules from the liver in the form of VLDL particles. So, has there been an overfilling of liver glycogen stores due to excessive activation of PC and GNG?
Was glucose production triggered after glycogen storage overflow?
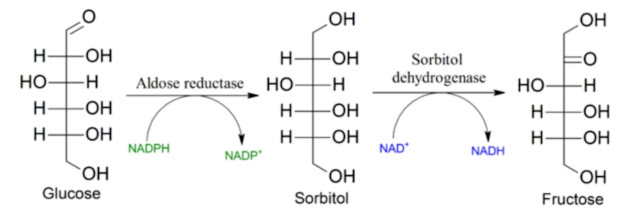
Did this trigger aldose reductase (AR) and fructose production and activation of the KHK enzyme?
Did KHK suppress the antioxidant system and GSH recycling?
Did the aldehyde 4-HNE form from linoleic acid through peroxidation and suppress the activity of ALDH2, and does further degradation of 4-HNE already occur via AR?
Does suppression of antioxidant protection fail to remove H2O2 and thus allow VLDL export and fat storage?
Due to poor antioxidant protection, are peroxidized fats also exported and cause immune activation and cellular senescence in adipose tissue? Does adipose tissue then become dysfunctional?
Let me repeat the first line: linoleic acid suppresses the export of acetyl-CoA molecules from the liver in the form of VLDL particles.
Oleic acid (green curve), which allows easy storage of fats into VLDL particles, does not increase acetyl-CoA and does not trigger excessive GNG, it leads to higher food consumption and fat storage in adipose tissue. It stores fats but does not trigger GNG or the polyol pathway, does not trigger sorbitol or fructose production, and does not activate the immune system in adipose tissue.
So why does soybean oil in the left graph suppress hunger and reduce food intake? By limiting fat export? By activating PPARα? By activating gluconeogenesis?
Yes, I think it's by activating gluconeogenesis.
Let’s take a closer look at what happens when gluconeogenesis is turned off—specifically when the hepatic enzyme pyruvate carboxylase (PC) is turned off.

Turning off gluconeogenesis significantly increases fat transport into mitochondria (CPT1).
I would note that this probably means that elevated acetyl-CoA levels, which activate gluconeogenesis, also trigger the liver polyol pathway and fructose production. What we see as a result is the removal of CPT1A and suppression of fat transport into the “furnace,” into mitochondria. What we observe is a typical effect of aldose reductase (AR) activation caused by aldehydes, specifically the product of linoleic acid peroxidation, the aldehyde 4-HNE. Turning off GNG manifests similarly to turning off KHK or AR—by shutting down the polyol pathway.

Turning off gluconeogenesis disrupts processes related to the breakdown and burning of excess amino acids.
Boom! That’s huge! So I have confirmation—I suspected it. From longevity studies, I predicted that insufficient activity of pyruvate carboxylase could be a problem when amino acids need to be processed. This was in connection with missing hydrogen sulfide production by the CSE enzyme, which produces pyruvate, and its carboxylation to oxaloacetate may be the solution to this problem.

Suppressing gluconeogenesis in the liver activates gluconeogenesis in the kidneys.
So this is confirmed. If 4-HNE suppresses S-sulfhydration of pyruvate carboxylase—i.e., suppresses gluconeogenesis—it will be replaced by glucose production in the kidneys. The consequence is known: increased fasting blood glucose as a result of renal processing of glycerol released during lipolysis along with free fatty acids from adipose tissue at night.

And finally, the most important point: turning off gluconeogenesis increases the liver’s susceptibility to oxidative stress and inflammation.
It leads to decreased NADPH recycling and suppression of antioxidant protection by lowering reduced glutathione levels. This increases lipid peroxidation, especially of linoleic and arachidonic acid, and leads to production of 4-HNE. This in turn further reduces PC activity and suppresses liver gluconeogenesis, closing the cycle. Gluconeogenesis is an important part of NADPH regeneration via the G6PD enzyme in the PPP pathway.

At first glance, turning off liver gluconeogenesis may appear beneficial—on a high-fat diet it leads to lower body weight, preserved insulin sensitivity, better fat burning, and ketogenesis. But it also leads to reduced ATP, higher lactate levels, worse antioxidant protection, greater sensitivity to oxidative stress, and higher peroxidation of polyunsaturated fats. The overall consequences of suppressing liver gluconeogenesis are therefore negative.
How do we get out of this? How can we restore the activity of the PC enzyme suppressed by 4-HNE molecules, and how can we restore proper liver gluconeogenesis if it has been halted by fat peroxidation? We’ll leave that for next time. For now, it’s enough that we probably have the culprit.
 |
| Proposed mechanism of hunger control |
Note:
As you can see from the diagram, to suppress hunger with vinegar (Acetate), it is necessary to use the time with low insulin levels, i.e. the time before meals.
After eating, when insulin level is high, vinegar can increase the formation of new fats and fat storage.
References:
Calorie restriction increases fatty acid synthesis and whole body fat oxidation rates


Comments
Post a Comment