Is Atherosclerotic Vascular Damage Related to Liver Damage?
I would like to loosely follow up on the previous post about conjugated linoleic acid (CLA) as a potential treatment for atherosclerosis. We saw that a 1% CLA mixture in the diet was able to almost completely heal blood vessels in mice within eight weeks; the previously formed atherosclerotic plaque in the aorta almost disappeared. This was not a slowing of plaque deposition processes, but its removal!

What could the mechanism be?
Could this work in humans as well?
In one older post, I showed how the number of unsaturated bonds in polyunsaturated fatty acids determines the degradation rate of apoB100 molecules, and therefore also the liver production of VLDL/LDL particles. The greater the susceptibility to peroxidation, the faster the degradation of apoB100 and the lower the export of fats and cholesterol from the liver.

Take a look at the following findings. Unlike the previous study, linoleic acid and palmitic acid behave the same way here. Human liver cells were used, which could explain the difference. Here, it is specifically CLA that suppresses apoB100 export, thereby reducing the export of triglycerides from the liver.

Limiting the export of fats from the liver usually activates their β-oxidation, increases hepatic acetyl-CoA levels, and thereby also gluconeogenesis. This leads to suppression of hunger, lower food intake, and reduced fat storage in adipose tissue. However, it may also lead to fatty liver if β-oxidation and gluconeogenesis are not activated via the transcription factor PPARα, e.g. in case of insufficient S-sulfhydration of enzymes.
Is there any relationship between fatty liver and atherosclerosis?
Yes, this study shows us that there could be a connection.

The immune system of people with liver damage is trained to attack apoB100 molecules.
I hypothesize that oxidative damage to apoB100 molecules, caused by peroxidation of polyunsaturated fats, should normally prevent their export from the liver and cause degradation of apoB100. However, damaged and fatty livers do not function properly and occasionally some of the oxidized apoB100 will leak out of the liver cells and into the bloodstream. This teaches the T-cells of the immune system to recognize damaged LDL particles.
After disruption of the vascular endothelium, for example through cellular senescence caused by impaired fat metabolism, LDL particles are used as a source of material for repairing the vessel. But there they are found by these “educated” T-cells, which begin to consume them. And vascular plaque forms — atherosclerosis.
But how is it possible that CLA can reverse this? I do not know; for now we can only speculate. CLA apparently can prevent the export of defective apoB100 molecules and prevent the export of peroxidized fats. The immune system then takes care of removing the oxidized ones, and if only undamaged VLDL/LDL particles enter the bloodstream, the blood vessels recover and clean themselves. What do you think? Could it work this way?
The question is whether the formation of oxLDL particles with damaged apoB100 molecules is linked only to damaged liver tissue, or whether it can also occur generally anywhere in the bloodstream. I cannot really imagine a mechanism by which CLA could prevent LDL oxidation other than by limiting their export from the liver. It therefore seems that oxLDL particles are formed specifically in the liver.
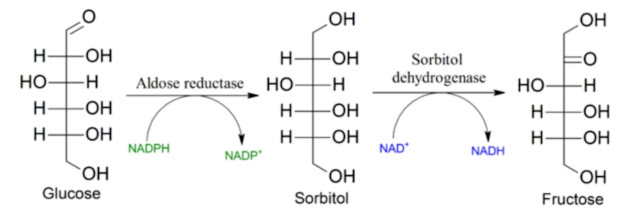
Let us revisit a statement from another older post, which discusses the issue of hepatic aldose reductase (AR) activation by peroxidized lipids, i.e., aldehydes such as 4-HNE or acetaldehyde derived from ethanol:

Quote
“In parallel with successful treatment of steatosis, aldose reductase inhibitor (ARI) suppressed ethanol-activated galactose metabolism and saturated fatty acid biosynthesis. Sorbitol in galactose metabolism and stearic acid in saturated fatty acid biosynthesis were potential biomarkers responsible for ethanol or ethanol plus AR inhibitor treatment. In vitro analysis confirmed that exogenous addition of sorbitol augmented ethanol-induced steatosis and stearic acid. These findings not only reveal metabolic patterns associated with disease and treatment, but also shed light on functional biomarkers contribute to AR inhibition therapy.”
Unquote
For now, this is my current idea — perhaps completely wrong — but as a working model I think it is fairly satisfactory. Over time we will see whether any contradictions or shortcomings of this model emerge.
An undeniably interesting question is whether approaches aimed at suppressing fatty liver, for example glycine supplementation, could also treat atherosclerosis and remove vascular plaque.
References:
Liver damage promotes pro-inflammatory T-cell responses against apolipoprotein B-100
The interplay between nonalcoholic fatty liver disease and atherosclerotic cardiovascular disease


Comments
Post a Comment