Is Alcoholic Liver Damage Really Caused by Alcohol?
Once again, I deliberately chose a provocative question for the title. It concerns the harmfulness of alcohol—specifically, ethanol itself. Do not understand this as me defending excessive or habitual alcohol consumption. No, alcohol consumption is addictive. But research conducted some time ago suggested that alcohol in small amounts might actually be beneficial, whereas now it is claimed that any amount of alcohol is harmful, even very small amounts. And that does not seem very likely to me, if I consider that alcohol can help activate the enzyme ALDH2, which appears to be very important for the detoxification of aldehydes derived from polyunsaturated oils, such as 4-HNE.
Why am I asking this question? Think about it! What if there existed some dietary component that could suppress or even repair liver damage during alcohol consumption. Wouldn’t that imply that the liver is being damaged by some other substance? It could not be alcohol itself! With this, I loosely follow up on a previous post on this topic.
And such a substance in the diet really does exist. It is the amino acid glycine. We have known this for quite a long time—over 20 years. That is, only some scientists know this; generally, it is not well known. Why?
For example, this study from 2003 beautifully demonstrates the protective effects of glycine. The study ran for 30 days on four groups of mice, and you can compare how glycine brought all monitored parameters in the alcohol-drinking group closer to those of the control group without alcohol.


But that is not all. In another study from 2004, we see an experiment where the liver was first damaged for 30 days by alcohol consumption, and then for another 30 days glycine was added along with alcohol. And it worked!


Note that the level of polyunsaturated fat peroxidation (TBARS) returned almost to the value of the control group after glycine was added.
How is that possible?
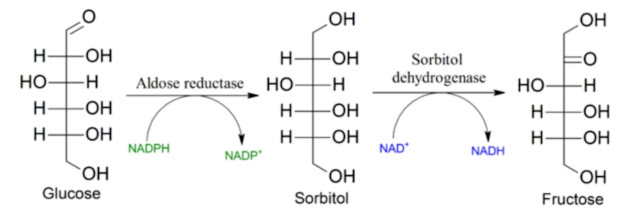
Let us now return to the vicious cycle of obesity, as I showed it in an older post. The key enzyme here is aldose reductase, AR—an enzyme that processes excess glucose into sorbitol, after which fructose is produced, which activates the enzyme KHK and oxidative stress.
If AR is almost inactive, increased glucose levels enhance GSH recycling through increased activity of the PPP pathway, thus acting as an antioxidant. But when AR is activated, high level of glucose triggers oxidative stress, a shift from oxidative phosphorylation to fermentation, activation of HIF1A, and pseudo-hypoxia.
All of this depends on the activity of aldose reductase: fat accumulation, inflammation, peroxidation of polyunsaturated fats. The AR enzyme is expressed by various aldehydes, including acetaldehyde—the product of alcohol metabolism—not only 4-hydroxy-2-nonenal (HNE) from linoleic fatty acid.


It is always the same situation: aldehydes activating aldose reductase. Alcohol is metabolized to acetaldehyde, which is then further processed by the enzyme ALDH2 into acetate. But part of it is processed via AR into signaling molecules, although so far I have not found any mention of what percentage. One outcome of AR activation will also be fructose production via the polyol pathway at high glucose levels. That is likely very important: a defensive response is triggered—oxidative stress and inflammation. If we disable the activity of the AR enzyme by any means, both inflammation and oxidative stress subside.

Glycine, or some product of its metabolism, works in the same way, as AR inhibitor. We know this from other research. Just as glycine can prevent cataract formation in diabetics, it can also suppress fatty liver and prevent liver damage during alcohol metabolism by suppressing AR activity.
So what causes liver damage? It is not alcohol directly, but high glucose levels together with the presence of aldehydes that could be responsible. It is the activation of aldose reductase! It does not matter whether the activation comes from peroxidized polyunsaturated oils, from alcohol, or from other toxic substances. AR activation leads to increased fructose production, KHK activation, oxidative stress, and chronic inflammation. Alcohol in small amounts does not activate AR. For alcohol to be harmful even in small amounts, other AR activators must probably be present—aldehydes from vegetable oils.
Does this manifest in studies of alcohol consumption in humans? Well, judge for yourself. Studies do claim that alcohol is always harmful. But we already know that if AR activity is suppressed, as it probably was several decades ago, even moderate alcohol consumption can reduce mortality risk. However, as AR activity increases over time with the rising content of linoleic acid in the body, alcohol also becomes more problematic. Thus it may happen that older studies in younger people show that alcohol reduces mortality risk, while newer follow-ups no longer show this—an increased burden of toxins from food and the environment activates AR, and additional burden only worsens the situation. This is how it came to be that moderate alcohol consumption at a younger age and abstinence at an older age leads to the longest lifespan, as shown by the green curve in the following graph.

References:
Glycine modulates hepatic lipid accumulation in alcohol-induced liver injury


Comments
Post a Comment