Obesity and Hydrogen Sulfide
In this post, I will try to summarize information from previous posts and studies and supplement it with the latest insights on the effect of enzymatic hydrogen sulfide (H2S) production on metabolism.

What do we already know?
Intestinal permeability
A high-fat diet with sugar promotes a composition of gut bacteria that produces a large amount of hydrogen sulfide. There is so much of it that this hydrogen sulfide deprives intestinal epithelial cells of ATP energy, blocks mitochondrial complex IV, and causes leaky gut. A high concentration of H2S damages metabolism.
Liver
With a high-fat diet containing sugar, the liver is burdened by endotoxins (LPS) from a leaky gut. These activate aldose reductase (AR), increasing the formation of H2O2 (ROS) in the liver. According to the already known scheme, this switches on fatty acid synthesis (DNL) as well as triglyceride (TG) production and activates their export further into the body, either to be burned for heat, to produce chemical energy (ATP), or to be stored in fat cells. This reaction is generally normal. If fat export works well, the liver is not damaged. At the same time, G6P and glycogen (GNG) production are activated via activation of pyruvate carboxylase (PC), but whether glucose or glycogen is produced depends on the activity of the enzyme G6Pase, which is modulated by amino acids and probably also by individual fatty acids. In the absence of essential amino acids, glucose production is preferred instead of glycogen formation. This leads to higher insulin levels, faster storage, and greater hunger, i.e., higher food intake. Presumably to ensure a sufficient supply of essential amino acids from food that contains little of them. This is normal regulation, which can also lead to obesity.
Blood
The digestive system and liver process eaten food into simpler components intended for use in the body or for storage. These intermediates are transported by the blood. Water-soluble substances travel in plasma; fats are packaged into lipoprotein particles of various sizes, into chylomicrons and VLDL. Short- and medium-chain fatty acids move similarly to long free fatty acids, i.e., bound to albumin, and can directly pass into cells; longer fatty acids are assisted by membrane proteins CD36. Fats from VLDL or chylomicrons require active lipase LPL for transfer into the cell, i.e., breakdown into individual fatty acids, because membranes are impermeable to triglycerides.
Adipose tissue
Fat storage is controlled by insulin, and this is at least as important as insulin’s control of blood glucose levels. Fat cells can either readily accept fats or resist them; they can become insulin resistant. In such a case, blood TG or even FFA levels increase if the liver has a problem exporting fats. If the liver cannot keep up with exporting TG from FFA, then H2O2 generated in the liver does not ensure fat export to the body but instead fatty liver develops.
Is the ability to store fat quickly bad and does it cause obesity?
This is a common misconception, even in many scientific studies. Researchers, for example, abruptly change the diet from low-fat to very high-fat (HFD) and thereby induce obesity. Then they examine different fat compositions to see which causes greater obesity. This is a completely misguided approach. Every adipose tissue has certain limits on how much fat it can safely accept at a given time. For this activity it needs, if possible, stable glucose levels and some insulin. Overload with glucose and insulin overwhelms all protective mechanisms; for example, high glucose levels stop the enzymes producing hydrogen sulfide (H2S). H2S is necessary for S-sulfhydration of enzymes involved in fat and glucose processing. If the activity of important enzymes is suppressed in this way, fat cells fall into cellular senescence manifested by insulin resistance and unwillingness to respond to external signals. Cells disconnect from the system and continuously accumulate or release fats regardless of external signals. But this has nothing to do with specific fats; it relates to the glucose levels reached during sudden overeating. It is enough to limit the rate of food intake so that the system is not overloaded, and the results will be completely different. For example, supplementing acetic acid/acetate is sufficient and alone can protect the liver and fat cells from overload. How exactly this works is a question; perhaps it is similar to alcohol, which has priority over all other fuels and slows the processing of carbohydrates, fats, and proteins. Acetate may do the same and additionally activates SIRT1/SIRT2 deacetylases, thus probably helping subsequently increase processing speed via more active enzymes. In conclusion, the ability to store fat quickly is healthy and is not the cause of obesity.
Thin outside, fat inside
The highest rate of fat storage occurs in adipose tissue shortly after weight loss. At this time it is also most vulnerable and easily overloaded by high glucose and insulin levels, thus losing H2S production. If you lose weight, keep in mind that any fat regain will cause even greater insulin resistance and senescence of adipose tissue. For the body to function, it will create new storage sites and store visceral fat. It can easily happen that peripheral adipose tissues no longer accept fat; you may be relatively lean, but fat will accumulate in organs, in the liver, in the pancreas, in the abdominal cavity. Beware of this. You can prevent it by supplementing vinegar, as described above.
High glucose levels block hydrogen sulfide production; aldehydes are responsible
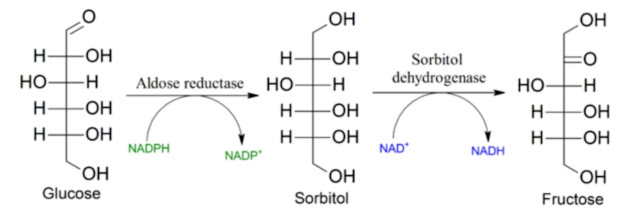
What mechanism causes elevated glucose and free fatty acid levels to so easily suppress enzymatic hydrogen sulfide production? One mechanism is fairly clear and I described it in connection with the vicious circle of obesity. It relates to peroxidation of linoleic acid into 4-HNE molecules. These molecules suppress the activity of the ALDH2 enzyme that removes aldehydes. Instead, the enzyme aldose reductase (AR) is activated. However, AR also functions as an emergency enzyme for processing glucose into sorbitol and subsequently into fructose if glucose levels are too high. In the absence of aldehydes, i.e., with sufficiently functional ALDH2, AR is minimally active and even high glucose levels do not lead to fructose formation and do not cause oxidative stress. On the contrary, they increase NADPH production via the PPP pathway, and glucose can thus behave as an antioxidant. The connection between ALDH2 activity and enzymatic H2S production is obvious and reciprocal. H2S molecules re-activate ALDH2, remove attached 4-HNE molecules, and ALDH2 subsequently eliminates them. Maintaining high ALDH2 activity is essential for preserving insulin sensitivity of adipose tissue and the ability to rapidly store fat without the risk of cellular senescence.
So how does obesity arise?
With every single episode of unmanaged overeating, you move toward cellular senescence of adipose and liver cells. While fat cells can probably be repaired by weight loss and protected by acetic acid, liver cell damage may be more permanent. This corresponds to the observation that after weight loss, adipose tissue has low and relatively healthy insulin resistance, but the liver still operates in an overload program, cannot stop exporting available fats to the body, cannot create more glycogen faster with lower fat export, and thus drives us to eat more. The ratio between fat export and glycogen formation is apparently crucial. The enzyme pyruvate carboxylase (PC) plays a major role here. This enzyme is activated by levels of acetyl-CoA molecules and S-sulfhydration, so it is only properly active if the resulting aldehydes are quickly removed. If they are not, it means higher food consumption and higher fat export into the body. How the body handles them is another question, because they can also be burned for heat and you simply become warmer.
So why aren’t calories burned as heat, but instead stored and you gain weight?
For heat to be produced, brown adipose tissue must function. It is usually activated by the hormone FGF21 during protein deficiency, by oxidative stress generated via succinate, and by the nervous system. But somewhere along this pathway hydrogen sulfide also plays a role; without it, it does not work. So again, if we think it through, high glucose levels suppress endogenous H2S production and thus limit heat generation in brown adipose tissue. How to solve this? By activating ALDH2 or suppressing AR? It suggests itself. Doesn’t alcohol activate the ALDH2 enzyme? And doesn’t it also trigger production of the hormone FGF21? And doesn’t that lead to warming of the organism? Think about it.
Solution?
You probably already know it: the solution is to activate the ALDH2 enzyme and suppress the AR and KHK enzymes, deactivate the polyol pathway at the beginning (AR) and also suppress the consequences of its activation (KHK). How to activate ALDH2 simply? I don’t know; alcohol suggests itself, but it is addictive. It would require some other activator. How to suppress AR we already know; supplementing the amino acid glycine in the diet can do it. How to suppress fructose effects we also know; a little of highly diluted vinegar is sufficient. We can further complement this with other short- and medium-chain fatty acids, which are contained, for example, in heavy cream. If we want to make the composition more similar to that of goat cream, we can also add MCT oil. We can add coconut oil as well. So now it should probably be easy to apply this in practice. Whether it works, we will see.
Hydrogen sulfide production in adipose tissue
I found an interesting paper addressing the effect of hydrogen sulfide on obesity. The discovery of hydrogen sulfide as a regulatory signal is not very old, and I have already written several posts about it. They concerned enzymatic hydrogen sulfide production, mainly in the liver. It activates, for example, deacetylation of enzymes, gluconeogenesis, etc. It usually increases enzyme activity. But how does hydrogen sulfide production affect fat cells?
In the previous figure, I would probably add glucose and free fatty acids (FFA) to the scheme. Instead of obesity, the main direct blockers of hydrogen sulfide formation in adipose tissue are precisely high glucose levels from processed foods and high FFA levels caused by adipose tissue’s reluctance to accept new fats.

Let us look at statistics of blood hydrogen sulfide levels and expression of the main hydrogen sulfide–producing enzymes (CSE/CTH, CBS and MPST) in visceral (VAT) and subcutaneous (SAT) adipose tissue depending on obesity (obese) and diabetes (T2D). From the figure above, it is clear that both obesity and diabetes reduce enzyme activity in adipose tissue, and this is associated with high blood glucose levels (IFG). If glucose levels are maintained within the normal range (NFG), hydrogen sulfide production is higher, see the figure below.

Blood hydrogen sulfide levels are directly proportional to obesity. Even though enzyme activity decreases with obesity, the more fat, the more hydrogen sulfide in the blood. Even in long-lasting obesity, elevated hydrogen sulfide levels persist. But if we are already obese, the worse the insulin resistance, the less hydrogen sulfide in the blood. Hydrogen sulfide production is probably not the cause of the problems, but rather an attempt at a solution. As if hydrogen sulfide had a protective effect. If it can be generated in adipose tissue via the enzymes CSE/CTH, CBS or MPST, then metabolically we will be better off.

So what does hydrogen sulfide control in adipose tissue? It facilitates fat formation and storage. It improves glucose entry and the assembly of fatty acids into triglyceride molecules and their storage in lipid droplets. It also promotes the formation and transformation of fatty acids into forms that are easily stored. If, for example, by blocking enzymes we reduce H2S production (PPG), fat storage decreases. At first glance this may seem good, but it is not. Fat cells without H2S activate cellular senescence during differentiation. Some cells stop storing; others, on the contrary, continue storing constantly. The biggest problem is that they stop responding to external signals. They will not store fat when needed, nor release fat when needed. This is reflected in worse blood parameters, high fasting glucose and insulin levels.

If I try to formulate the overall picture: if adipose tissue accepts fat, it is good for blood parameters. What we eat is quickly stored for later. That is how it should be. The catch is that high glucose or free fatty acid levels suppress the activity of enzymes producing hydrogen sulfide. We have already shown this here. A large and rapid fuel surplus that raises glucose levels is not good for adipose tissue. It relatively quickly slows fat storage, which worsens blood parameters. But adipose tissue is not to blame; it is merely defending itself against being flooded with excess fuel.

Why did adipose cells become overloaded in the first place? A large uncontrolled hunger? Or bad food? Too rapid conversion into glucose?
Yes, it is still the same thing: too high a rate of food processing. Natural food is usually low in concentration. Try overeating on wild strawberries or nuts picked directly from the tree. I do not mean already shelled and processed to be as tasty as possible. In their natural form. Even meat cannot be eaten too quickly if it contains connective tissue. The biggest problem with processed foods is their “pre-digestion,” i.e., processing into a mass that does not even need to be chewed.
So the lesson might be: eat as slowly as possible, do not rush, think about your liver and adipose tissue; they have their limits. Give them enough time by reducing the rate of calorie intake.
References:
THE RELEVANCE OF HYDROGEN SULFIDE (H2S) IN OBESITY AND ADIPOSE TISSUE PHYSIOLOGY


Comments
Post a Comment