Can MCT Oils Reduce the Omega-6 Content in Membranes?
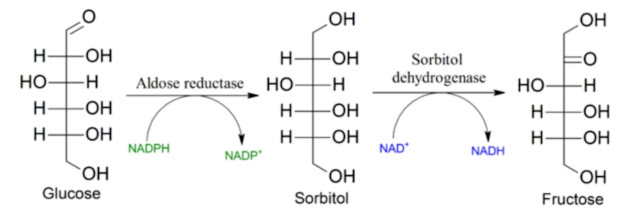
You probably already know this. Oxidative stress of any kind triggers the activity of enzymes called phospholipases, especially iPLA2γ, which releases oxidized polyunsaturated fats from the mitochondrial membrane. This is how cells monitor their condition and oxidative stress, and the released oxidized products derived from omega-6 linoleic acid (LA/ARA, e.g., 4-HNE) serve as signals for many processes. For example, they can also trigger chronic inflammation by activating aldose reductase (AR) and the polyol pathway. Elevated glucose levels (HG), when the enzyme ALDH2 functions insufficiently and 4-HNE molecules are attached to it, become problematic and instead of correcting oxidative stress they deepen it further. The missing ALDH2 activity can be restored using H2S (NaHS was used here) or by activating the CSE enzyme (e.g., by restricting methionine and cysteine in the diet).

I have many posts about this here; most of them concern liver cells or pancreatic cells, and therefore also insulin secretion. But if the fats released from membranes come from omega-3 fatty acids (DHA, EPA) or, even better, from the monounsaturated oleic acid (OA), the reaction is different and not inflammatory. Our wish is therefore to have more oleic acid and less linoleic acid in our membranes. But how can this be achieved?
From the title you probably guess where I am going—yes, what if higher consumption of medium-chain triglycerides (MCT) could replace part of the omega-6 arachidonic acid (ARA) molecules embedded in membrane phospholipids with molecules of the safe oleic acid (OA)? That would be good, wouldn’t it? We know that a low-fat carbohydrate diet can do this. But in a situation with increased activity of the AR enzyme it produces sorbitol and fructose. You don’t want that! What if a similar replacement of molecules in membranes could be achieved more safely using MCT oil—even in an environment with active aldose reductase (AR)? For now I don’t know. Let’s look at an older study. I linked to it a long time ago.
This is a study of dietary effects in healthy men who were given 50% more calories in food for one week, examining the effect of fats. The food contained 40% fat in two forms: either as LCT (long-chain triglycerides), fats containing mainly oleic acid C18:1 and linoleic acid C18:2, or as MCT (medium-chain triglycerides), fats containing mainly fatty acids C8:0 and C10:0. MCT oils are sold as dietary supplements and are easy to obtain.

Let’s show the most interesting figure: the content of free fatty acids with lengths of 18 to 20 carbons (C18–C20). Fats enter cells in the form of free fatty acids. From previous posts we already know that the indicator of proper fat processing is exclusively the level of non-esterified oleic acid. It regulates storage in adipose tissue, export of fats from the liver, and the addition of fat cells through differentiation of preadipocytes. Another indicator is the level of palmitic acid C16, but that is no longer a regulatory signal—it is an emergency signal. An increased C16 level means something is seriously wrong. Now let’s look at some graphs from the study.

First, let’s look at what vegetable oils (LCT) do. On the first day (day 1) we see a relatively high and stable level of C18 that does not change even after a meal. After a week of overeating, a reaction to the meal appears. Overeating increased fat storage and reduced the release of free fatty acids for burning; fats are stored while carbohydrates are used more. Insulin during the meal suppressed the availability of fats as fuel—but only for a short time. After four hours the situation is the opposite: the level of long-chain fatty acids rises considerably. We are mainly interested in oleic acid C18:1, which stimulates the formation of new fat cells. We see that the body adapts to excess calories and signals the need to increase the number of fat cells through increased levels of oleic acid. The level of palmitic acid did not increase, so an emergency state did not occur. The fat cells are functioning.

This is the most interesting graph, demonstrating fundamental changes in fat metabolism when the fats are medium-chain triglycerides (MCT, C6–C12). Something fundamental happened already on the first day, after the first meal with MCT oil. The drop in oleic and linoleic acid levels is very marked and rapid—from 60 μg/ml to 20 μg/ml in 2 hours! Moreover, this level remained stable throughout the experiment. No signal arose for the formation of new adipocytes, nor for enlargement of adipose tissue or fat cells. What happened?

What happened can be seen in another graph. MCT oils greatly increased triglyceride levels. That means free fatty acids were combined in the liver into triglycerides and sent for storage or immediate use. Low levels of free fatty acids (FFA, NEFA) mean that all fats released by lipolysis were processed in time and are not accumulating. Although high triglycerides may seem bad—since they are a marker of metabolic disorders—once fats are in the blood, be sure that in the form of triglycerides they are relatively safe, while in the form of FFA they are not. Moving oleic and linoleic acid into triglycerides is a good move.

We can look at the specific composition, but unfortunately here the authors mixed apples and oranges. They combined oleic acid with linoleic acid into a single number. That creates a problem for evaluation. Fortunately, in the text they list them separately.
Citation from the study:
"Analysis of triglyceride fatty acids on the packed column revealed that C18:1 was increased (32.1% vs 30.4%) while C18:2 was markedly decreased (8.3% vs 35.6 %) in MCT as compared to LCT feeding. Considering that fasting triglycerides were 2.5-fold higher when subjects were on MCT compared to when they consumed LCT diets, these data suggest that the absolute amounts of all triglyceride fatty acids except C18:2 and C20:4 were increased with MCT feeding. That is, in addition to an increase in triglyceride MCFAs (which were essentially absent from triglycerides during LCT feeding), C14:0 increased approximately 6-fold, C16:0 and 16:1 increased approximately 4-fold, C18:0 increased approximately 3-fold, and C18:1 increased approximately 2.5-fold compared with LCT feeding."
End of citation
Let’s summarize. MCT oils from the diet go directly to the liver, where they increase the level of acetyl-CoA molecules and trigger de novo lipogenesis (DNL), the formation of saturated and monounsaturated fats. They therefore fundamentally change the ratios of fatty acids in triglycerides. They produce palmitic acid, but it is elongated and desaturated into oleic acid. At the same time, MCT oils contain almost no linoleic acid. They therefore reduce the relative proportion of linoleic and arachidonic acid in triglycerides that the liver sends to the body for storage or metabolism into ATP energy. In this study a reduction of the relative LA content in triglycerides by about 75% (from 35% to 8%) was observed. This could be very interesting if your own fat stores contain a lot of linoleic and arachidonic acid.

Will this change also be reflected in phospholipids? As we see above, not much in this short-term study. The C18:0 level decreased somewhat, but we do not know whether this is significant. In my view the biggest change is a 30% increase in C22:6, i.e., DHA, a long omega-3. That could be important because DHA limits fat entry into the cell by suppressing CD36 and thus allows simultaneous processing of fats and carbohydrates without causing metabolic problems. It would be interesting to observe the longer-term effect—how the exchange of fatty acids in phospholipids manifests itself over the long term and without overeating. This study does not answer that.
MCT oils increase immediate energy expenditure as heat. This is usually associated with an increase in oxidative stress. This study did not examine that, but from other studies we know that long polyunsaturated fats eventually reduce heat energy expenditure, probably because they undergo peroxidation in an oxidative environment. I attribute this specifically to the effects of 4-HNE on enzymes—slowing their function—which results in a shortage of H2S molecules and insufficient S-sulfhydration of enzymes. Could MCT oils in the diet help restore H2S production? One of the resulting products of sulfur amino acid metabolism is pyruvate. High levels of unprocessed pyruvate can therefore block H2S formation. Pyruvate can be processed either into lactate, acetyl-CoA, or oxaloacetate. We know that processes of new fat formation (DNL) and new glucose formation (GNG) are triggered together, for example through PPARα (which triggers fat burning in peroxisomes, production of H2O2 and acetate), increased H2O2 production—i.e., oxidative stress (usually H2O2)—and oleic acid created for example from acetate/acetyl-CoA through DNL.
The balance between DNL and GNG processes is very important. A higher level of acetyl-CoA triggers GNG (via the PC enzyme and consumes pyruvate), and DNL consumes acetyl-CoA; therefore easy fat storage suppresses GNG and lowers glucose levels. Difficult and slow fat storage increases acetyl-CoA levels and supports GNG and glycogen production, sometimes even glucose production. Everything seems connected to everything else so that it can be regulated only as a whole.
It is difficult to separate individual processes from each other; doing so can easily lead to misleading conclusions and recommendations. MCT oils, through their rapid metabolism, apparently increase acetyl-CoA levels and thus trigger both GNG and DNL. But they also change the ratio between GNG and DNL. If the meal contains exclusively short- and medium-chain fatty acids without long chains, metabolically it resembles a low-fat carbohydrate diet. DNL is activated to convert medium chains into oleic acid suitable for storage. This is complemented by GNG up to G6P and glycogen formation. Sugars—glucose and fructose—enter the process here. While fructose does not suppress gluconeogenesis, glucose does. In this way the amount of food that needs to be eaten is controlled. Consumption of MCTs therefore does not lead to overeating, unless gluconeogenesis is switched off. This can be switched off via PPARα, as we have already seen.
What happens when PPARα is switched off in the liver (Pparαhep-/-) or in the whole organism (Pparα-/-)? What can be inferred from studies?

Interestingly, the connection between PPARα and GNG is not widely known. As a result, the authors of a study investigating exactly this factor do not mention gluconeogenesis at all. They do not examine it at all. Not at all!

Look at the figure above showing how fasting glucose levels change in mice with PPARα switched off only in the liver (red), in the whole organism (blue), and without the switch-off (gray). This is for two types of diet: a standard low-fat diet (CTRL) and a high-fat diet with lard and sugar D12492 (HFD). The high-fat diet clearly supports GNG even in the control group (WT HFD). When you switch off GNG in the liver, fasting glucose decreases; when you switch off GNG in the whole body, glucose completely normalizes—surprisingly even during the OGTT test (AUC)! Do you see that too? In the entire study there is nothing about gluconeogenesis, even though they examined all genes and fatty acids, all pathways, etc. What kind of strange science is this nowadays? I am a layperson—why should I be the one advising them? (Addenum: PPARα governs glycerol metabolism)
- Why, under a standard mouse diet, does switching off PPARα in the liver lead to increased GNG in another part of the body and to higher glucose levels?
- GNG in other parts of the body doesn't produce glycogen, so does it raise blood glucose and insulin secretion more than liver GNG?
- Why does cholesterol synthesis increase?
- Did lipolysis increase so much that it was necessary to trigger GNG in another part of the body?
- Is cholesterol synthesis a solution to metabolic problems related to reduced GNG in the liver?
- Is it related to amino acid breakdown?
Interestingly, the authors of this study apparently did not even ask any of these questions. We do not know why, nor which other organ had to replace hepatic GNG.

Gluconeogenesis in the fasting state regulates insulin levels and reduces lipolysis—the release of fats from adipose tissue. I assume that when GNG in the liver is switched off, the level of, for example, oleic or linoleic acid increases and thus increases GNG in, for example, the kidneys. That could explain the higher blood glucose level in the CTRL Pparαhep-/- group.
But why the higher cholesterol? I once had a post about this. It showed that a lack of TCA cycle products for the malate–aspartate shuttle leads, when mitochondrial complex I is restricted, to increased cholesterol synthesis in the liver. It is a solution to a problem—a problem with exporting electrons from mitochondria. It is solved by increased production and export of cholesterol from mitochondria.
And what did the complete shutdown of PPARα do? Did it reduce the production of new fats via DNL? Did the amount of FFA—free oleic acid in the blood—decrease? I would say yes. Switching off GNG probably does not matter under a chow diet because DNL in adipose tissue is also not activated, which is controlled by oleic acid. Nevertheless, fats are stored very easily due to low insulin resistance in adipose tissue. Everything is connected to everything.
What can be said in conclusion?
Medium-chain fats (MCT) can be a useful dietary supplement. In some foods they are present in fairly large amounts, for example in butter or coconut oil. In others they are completely absent. In our toxic environment, and due to auto-oxidation of omega-6 oils, an imbalance apparently arises between the formation/storage of glycogen and the formation/storage of fats. Insufficient S-sulfhydration of enzymes (PC, ALDH2) occurs, causing this imbalance between GNG and DNL. There must be cooperation and coordination between these processes; otherwise it leads to imbalance in food intake and storage, and to obesity. That is how it appears to me. Short- and medium-chain fats—SCFAs and MCT oils—may help restore this disrupted balance by supporting not only the new formation of oleic acid as the main regulator of fat storage, but also the formation of glycogen as an indicator of how much food has been eaten, which oleic acid itself or olive oil alone cannot achieve. Moreover, over a longer period they may probably replace omega-6 polyunsaturated fats in membrane phospholipids with newly formed, safe, and stable oleic acid.
References:
Changes in blood lipids during six days overfeeding with medium or long chain triglycerides
Hepatocyte-specific deletion of Pparα promotes NAFLD in the context of obesity
PPARα governs glycerol metabolism


Comments
Post a Comment