What Determines Fasting Blood Glucose?
Do not expect me to answer the question in the title with certainty. You probably understand that the body is very complex and nothing is that simple; moreover, each of us is different, and when something works for one person it may not work for someone else. So let’s get back to reality, we will look at two studies and I will try to comment on the observed results in my own way. Take it as you wish—believe it or not, that is up to you.
The answer to the basic question “What is good and what is bad?” may not be easy at all. Is easy and rapid fat storage good or bad? Recently it has become increasingly clear that easy and rapid storage of fat in adipose tissue is a sign of good metabolism and does not lead to obesity. Obesity is determined by overeating, the easy availability of overly tasty and overly digestible food, and insufficient satiety signaling. The ability to quickly store these surpluses without damaging metabolism determines the health of adipose tissue; unhealthy adipose tissue may have a smaller volume but can cause greater damage in the body, for example diabetes. Being thin does not always mean being healthier. It is therefore difficult to determine what is good and what is bad.

Let us now go back a little. I have already shown this image once. On the left is fasting glycemia for three groups of mice: with active factor PPARα in the whole body, with Pparαhep-/- switched off in the liver, and with Pparα-/- switched off in the whole body. I pointed mainly to the HFD bars, that is under a high-fat diet (HFD). Why is fasting glycemia increased with a high-fat diet and why does switching off the PPARα factor lead to normalization of glucose levels and even cholesterol? It looks like an improvement, doesn’t it? But do you know what it does during fasting?
Let us look at another similar study that examined liver fat accumulation during fasting, when the activity of the PPARα factor is highest. It seems that PPARα determines the behavior of the body when it operates from its own reserves. The time courses during 24 hours of fasting in mice are interesting. Let us look, for example, at the factor FGF21, which seems to be very important.
Quote from my older post:
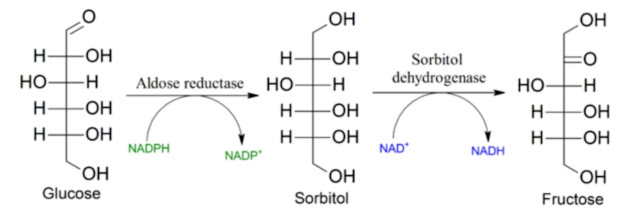
“If the expression of the gene for the production of FGF21 is genetically increased even in the absence of food deficiency, then the pathway of gluconeogenesis as well as beta-oxidation of fats, the TCA cycle, and ketogenesis are activated; even the PPP pathway and the production of NADPH for restoring reduced glutathione are activated more. Thus fat burning is supported and liver glycogen stores are spared, but its formation is also slowed. The enzyme G6Pase/G6PD is activated. As we already know, this enables rapid phosphorylation of glucose, prevents fructose formation, and leads to lower glycogen production, thus suppressing insulin resistance.”
And we can see all of this in the following figure during activation of FGF21 (Ad FGF21). But it just didn't help when PPARα was simultaneously switched off. Is PPARα even more important than FGF21? When PPARα is switched off in mice during fasting, blood glucose (Glycemia) and body temperature drop sharply, below 32 °C.

So what does PPARα control? And why only during fasting?
Fasting is characterized by a low level of insulin. This triggers lipolysis and the release of free fatty acids (FFA) and glycerol into the blood. If the liver is functioning properly, FFA activate PPARα and thereby GNG consumes the released glycerol to form new triglycerides and glycogen. Blood glucose levels are therefore low during fasting. Excess glucose is consumed. If by chance there is more glucose than is consumed, it can be stored as glycogen.
Because the PPARα factor controls gluconeogenesis from glycerol, and because glycerol is produced as a product of lipolysis of triglycerides stored in adipose tissue, switching it off mainly has an effect in a state when stored fats are the energy source. It is precisely the combination of released free fatty acids, which activate PPARα, and higher levels of glycerol that triggers gluconeogenesis, which stabilizes blood glucose levels during fasting.
Here we come to the issue of the difference between hepatic gluconeogenesis and renal gluconeogenesis. Although it may seem that it does not matter where GNG occurs, from the previous post and the first image above it is clear that it definitely does matter. Switching off PPARα in the liver suppresses the production of G6P from glycerol, which does not necessarily have to be used for glucose production but can also be stored as liver glycogen. The kidneys cannot do this. If the kidneys replace hepatic GNG, fasting blood glucose levels increase.

The liver controls fasting lipolysis not only through blood glucose levels but probably also through production of the hormone FGF21. The activity of PPARα increases during fasting, that is at low insulin levels and active lipolysis, probably through the availability of FFA. This certainly also increases the availability of blood glycerol. This leads to greater gluconeogenesis and to the production of FGF21. If PPARα in the liver is switched off, neither FGF21 nor ketone bodies are produced and lipolysis is also suppressed. Insufficiently activated PPARα in the liver therefore not only increases blood glucose through activation of GNG in the kidneys but also suppresses lipolysis and causes a lack of fuel during fasting. This could also explain the observed increase in total body weight in one of the models with suppressed PPARα in the liver and the decrease in body temperature during fasting.
I will venture a hypothesis that increased morning glycemia could be a product of renal gluconeogenesis from glycerol released overnight from adipose tissues if the liver does not function well. To reduce it, it might be sufficient to activate hepatic gluconeogenesis more, that is hepatic PPARα and the production of FGF21.

It seems that liver damage can be easily accelerated precisely by switching off PPARα. A high-fat diet is not even necessary. Notice that switching it off only in the liver (Pparαhep-/-) leads to suppression of fat metabolism and ketogenesis is suppressed. Fats apparently do not enter beta-oxidation and the TCA cycle at all. They are incorporated into triglycerides or circulate as free fatty acids (FFA); they are not burned and leave liver cells free to process glucose. This leads to low insulin resistance. Could it be caused by low oxidative stress?
Is it due to low or high production of H₂O₂, low or high oxidative stress?
I already discussed this once in a post about saturated fats, specifically about palmitic acid C16:0 (PA), why exactly this acid is not and cannot be the cause of metabolic problems, although it may appear so at first glance.
It is because the oxidative stress that palmitic acid directly causes has a regulatory function. Oxidative stress sets the proper gene expression for the production of enzymes for elongation to stearic acid (SA) and for desaturation to oleic acid (OA), which in turn reduces H₂O₂ production. Oxidative stress is therefore controlled and stabilized at some optimal value. For this to work, however, a functional antioxidant system based on glutathione (GSH) is also required. If GSH recycling does not work, the regulation of stress cannot function properly either.
The whole process is controlled through the JUN/JNK pathway, which responds to H₂O₂ and controls insulin sensitivity. More stress means greater insulin resistance and less glucose entering the cell. In the case of fat burning this is the correct response.
If we therefore have the information that switching off PPARα in the liver reduces insulin resistance of liver cells, then this is consistent with stress management, because switching off PPARα reduces the formation of H₂O₂ by limiting fat burning in mitochondria and especially in peroxisomes. The latter are known producers of hydrogen peroxide. Suppressing PPARα therefore suppresses fat burning and reduces H₂O₂ levels, reducing insulin resistance. For the production of ATP energy, glucose will therefore be preferentially used, which during combustion produces less H₂O₂ and moreover allows easy recycling of the antioxidant GSH via recycling of NADPH in the PPP pathway. All of this would fit. Why is it not good? Reducing oxidative stress should be good, shouldn’t it? It seems that not always.

It is all somewhat complicated, isn’t it? What should we take from it?
Fatty liver can apparently be triggered by a number of mechanisms. In this study it is caused by low oxidative stress during fasting, which does not allow the liver to export triglycerides further into the body, so they remain in the liver and cause its fat accumulation. This is probably a completely different mechanism from, for example, choline deficiency or fatty liver induced by endotoxins from the digestive system, which trigger aldose reductase (AR), inflammation, and high oxidative stress.
And one more bombshell at the end!
Look again at the first image above, really carefully. A fatty mouse diet with lard and sugar (HFD, D12492) activates gluconeogenesis in the liver and kidneys even outside fasting.
Switching off PPARα completely normalizes blood glucose levels on a high-fat diet.
Do you still not see it?
Do you think all fats do this or only some? Could it be, for example, the omega-6 linoleic acid?

Could this be the answer? Does linoleic acid released by lipolysis from adipose tissue activate gluconeogenesis in the kidneys even outside fasting? If so, we have here a source of problems even without peroxidation to 4-HNE. For this mechanism to operate, the mere presence of non-peroxidized linoleic acid is sufficient.
Is activation of hepatic PPARα by linoleic acid outside fasting also the mechanism by which linoleic acid reduces cholesterol production?
(Update, continue reading here)


Comments
Post a Comment