Are plant seed oils a medicine or a poison?
It is strange. Mechanistically, it is clear that dietary linoleic acid is associated with increased oxidative stress and odd auto-oxidation products such as 4-HNE, which is a molecule that binds to enzymes in a way that prevents them from functioning properly. It even prevents its own removal, so its concentration increases, and it should be easy to arrange a simple experiment: give one group of people more linoleic acid in the diet than the control group receives, and the result should be a clear difference. But that is not how it works.
Thus, for example, when Tucker Goodrich, a well-known blogger and proponent of the theory about the harmfulness of linoleic acid, is asked on the X network to support with a human study that linoleic acid causes inflammation, he presents a study with this conclusion:
"Our meta-analysis suggested that increasing dietary LA intake does not have a significant effect on the blood concentrations of inflammatory markers. However, the extent of change in dietary LA intake might affect the effect of LA supplementation on CRP."
So how is it then—does it harm or not? But what if it does not cause inflammation and perhaps heals something? Plant polyunsaturated oils lower cholesterol; there is no dispute about that. Do they therefore reduce the probability of cardiovascular disease?

Probably not either; perhaps they worsen the probability of vascular damage. The result of the well-known Minnesota Coronary Experiment was re-evaluated: the probability of death from any cause was higher on a diet with plant oils than on the control diet. The authors state:
"Available evidence from randomized controlled trials shows that replacement of saturated fat in the diet with linoleic acid effectively lowers serum cholesterol but does not support the hypothesis that this translates to a lower risk of death from coronary heart disease or all causes. Findings from the Minnesota Coronary Experiment add to growing evidence that incomplete publication has contributed to overestimation of the benefits of replacing saturated fat with vegetable oils rich in linoleic acid."

So it is probably a bit more complicated; something must be different. But how? Are plant oils a medicine or a poison for humans? Or are they neutral?
I will try to untangle this mystery a bit, from my lay perspective. We are only at the beginning, but I have nevertheless found something.
We will start with uric acid; it has already once proven itself to be a good indicator of longevity, which may help us. Lately I attach great importance to lifelong studies of metabolism in animals and humans. Short-term studies often mask long-term problems behind short-term results and are therefore very misleading.

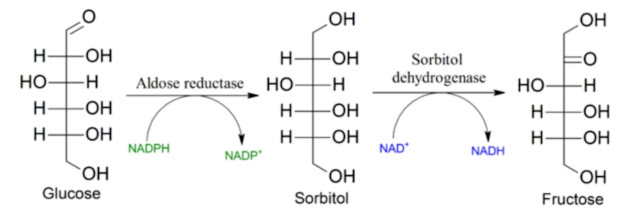
Seed oils promote the excretion of uric acid, lowering its level in the blood. This could mask a problem in which the auto-oxidation product of linoleic acid, 4-HNE, expresses AR and thus amplifies the production of fructose from glucose via the polyol pathway. This increases oxidative stress and the production of uric acid. But because excretion simultaneously improves, the level of uric acid in the blood decreases and the effect of endogenous fructose production is suppressed. Thus a compensatory effect is created, which sometimes may work and sometimes may not.

Another compensatory effect may be created by intestinal bacteria that, in the presence of polyunsaturated oils, produce acetate. This can also compensate for the effect of endogenous fructose production. Compensation, however, is not a solution to the cause, which is probably why the results of dietary studies are contradictory; they are highly dependent on parameters other than those being monitored. Nobody measures acetate production in the intestines and liver. Nobody determines H₂S production in the intestines and CSE activity in the liver.
So, so far nothing. We simply do not know. Let’s move on.
Is it even possible to increase or decrease the total content of omega-6 in structural products, in cholesteryl esters, in LDL? It appears that not much.
Let us look at a study in healthy people, young women, who were given for two weeks at a diets with 0%, 4%, and 20% linoleic acid in a special liquid diet. The study was well controlled and randomized, but only short-term. Never mind—the trends are clearly visible anyway. With increasing consumption of linoleic acid, the activity of the D6D desaturase decreases, and thus the production of arachidonic acid is reduced. The total amount therefore does not change much.


The conclusion is that the total amount of incorporated omega-6 fats is stabilized, and only 4% of total caloric intake from linoleic acid is sufficient to meet needs. There really is no need for more; higher amounts only deactivate the D6D enzyme and reduce not only the production of arachidonic acid, but also the production of long omega-3s from plant ALA, thereby reducing the percentage of long-chain omega-3 fats in favor of the shorter linoleic acid. The total amount of PUFA is the same, so the ratios worsen with higher intake. This corresponds beautifully with the results of studies in mice. More plant omega-6 fats mean fewer long-chain omega-3s.

The excess is stored or released as free fatty acids to be burned. If oxidative phosphorylation functions well—i.e., low activity of the polyol pathway and low fructose production, not active fermentation or a state of pseudohypoxia—then probably nothing negative happens. All fats are nicely burned under full antioxidant protection. It can be assumed that under such circumstances linoleic acid is not harmful. We observed this in animal models with fructose metabolism switched off (KHK-KO).
What provisional conclusion can be drawn from this? In animal models that could be trusted, I have so far seen no positive results of high consumption of linoleic acid in vegetable oils. It is true that in some cases the production of short-chain fatty acids by intestinal bacteria may increase. This could protect the digestive tract, the liver, and adipose tissue. But why do this with the risk of increased oxidative stress and heightened chronic inflammation? We already know a better way. Short-chain fatty acids can be supplemented directly, as vinegar or butyrate (in cream/butter). And increased excretion of uric acid can be ensured by supplementing glycine. It simultaneously suppresses the polyol pathway and endogenous fructose production. This makes it possible to strengthen antioxidant protection and suppress inflammation. So we have a far safer solution; it is unnecessary and probably even harmful to increase linoleic acid consumption.
References:
Inverse association of dietary consumption of n3 and n6 fatty acids with hyperuricemia among adults
Impact of linoleic acid intake on arachidonic acid formation and eicosanoid biosynthesis in humans


Comments
Post a Comment